Yesterday, I had a very long and emotionally draining meeting with the Radiologist Oncologist who will be treating me with radiation. He was a very nice, informative doctor who took the time (2 1/2 hours actually) to fully and completely explain the different options, positions as well as the pros/cons involved with this very important decision. I will attempt to share some of that in this post. For those who don’t really want to read all the details, I will share here that I will need to endure 6 weeks of radiation, 5 days a week. This will not start for another month or so … giving me time to heal from my surgery 2 weeks ago. Also, my cancer has been staged as a 1A breast cancer.
First he went over the details of my particular diagnosis. The fact that I had microscopic evidence of the invasive cancer (even though none was found in the tissue that was removed during surgery) changes the way I will be treated. He must treat me for the more aggressive form, to ensure the optimum results going forward (i.e. a long, healthy life with the least risk of developing a new breast cancer or having a cancer recurrence). There are several regimens that are practiced, that on the surface give the same outcome. I don’t understand all the terminology he used, but was able to understand that the shorter radiation treatment (4 weeks) would be with a higher concentrated radiation beam or voltage. (As I said, I don’t understand the terms used … but the shorter treatment is with a higher concentration of radiation or something like that.) He used “267” in the shorter treatment along with a hypofractionation term; and then “200” in the longer treatment with a conventionally fractionated three-dimensional external-beam radiotherapy. Basically the end result is that he believes the longer, 6 week radiation program, with the lower “200” conventional beam would be better for my case, given the microscopic invasive cancer found in the biopsy. The invasive cancer being present, even if only from the biopsy, dramatically changes the way one is treated, as it’s recurrence risk is much higher than the DCIS only would have been.
Then he spent time explaining how the 6 weeks will start to affect me. For the first 3 – 3 1/2 weeks, I will likely not have any change in how I’m feeling. At around the 3 1/2 – 4 week mark, fatigue will start setting in. He explained this to be more like going to bed an hour earlier than normal, or taking a nap in the middle of the day (if i didn’t work). This would be something I experience every day during my treatment phase. Around week 4, I’ll start to notice skin dryness; week 5 I’ll notice the skin becoming pink and starting to itch, then week 6 some patients will have some small peeling – similar to the peeling when you get a bad sunburn.
For the first 5 weeks, I’ll have radiation of the entire breast; then for the final week, they change and focus a more concentrated beam at the tumor area … which will minimize some of the skin symptoms experienced the first 5 weeks. This includes at the 7-10 day mark, following week 5, I will start bouncing back a bit from the fatigue and a lot of the other affected skin changes will start looking and feeling better. During the final week of treatment, however, I may also notice a ‘tan’ appear on the breast. This is typically only a shade or two darker than the rest of my skin … and will hopefully lighten over time (meaning years).
Next we went over the typical chronic concerns involved with radiation:
- Skin changes
- Heart impact
- Lung impact
- 2nd cancer diagnosis over lifetime
As you can imagine, this was a long in-depth discussion that involved how different body positioning during radiation treatment impacts items 2-4 above.
There are two different positions that can be used for breast cancer radiation treatment.
- There is the “supine” position, where you are on your back with a wedge under your back/head at a 10-15 degree incline, as well as a round pillow roll under the knees and your arms are above your head. In this position, they are able to radiate the entire breast (including the nodal area under the armpits). They also perform x-ray / CT scanning to know the exact position of the heart and lungs. They will put a ‘heart block’ to shield the beam from the heart, and will minimize the amount of the lung in the range of the radiation beam. (For some people, their lungs are set further back from their breastbone, so none of the lung is in the beam … but some other people’s lung is right up against the breastbone, so a small amount is in the range of the beam. They can utilize a technique called “DIBH” — basically an intermittent breath hold, that can further protect the lung during treatment. This position also allows better consistency in ensuring they radiate the same area every day for the duration of treatment.
- There is a “prone” position, where you are on a table (similar to the one where my breast biopsy was performed) on your stomach and your breast hangs through a hole. The radiation beams are shot under the table. I had incorrectly thought that this position would protect my heart and lungs from the radiation, but that is not the case … it provides no protection that way. Additionally, they are unable to radiate the entire breast in this position … as the nodal area under the armpits and center area, closest to the breastbone, would be blocked by the table. Additionally, they do not have the ability for exacting precision in consistently radiating the same exact area, as one can never always be in the same exact position / angle / tilt on the table every day for 6 weeks. Finally, they are not able to do the x-ray / CT scanning to perform the heart block in this position the same way either.
Another radiation technique is proton therapy. While that also sounded like a great option, for my case, he does not recommend it. Those beams are aimed straight on, as opposed to angular across the breast (i.e. left to right) and there would not be the same protection for the heart/lung, as they can use for the supine positioning.
Finally, he explained that the lifetime increased risk of a new cancer differs based on chemotherapy treatment and radiation treatment. Your increased risk of new or recurring cancer is largest with chemotherapy in the first 10 years following diagnosis. With radiation, your increased risk of a new or recurring cancer is largest at the 30 year mark, however, that increased risk is small, only 0-2%. Still – good information to know and be aware of.
WHEW! That’s a lot of information!! I have time to think about all of this and come up with a choice on which I’d like to pursue, as I still have another month or so before the radiation will start, so I can heal from my surgery. I’ll be praying for God’s guidance so I make the best decision.
Thank you for your continued prayers, cards, email messages, and gifts. I love and appreciate all of you so very much. Until next time … Happy New Year!!!



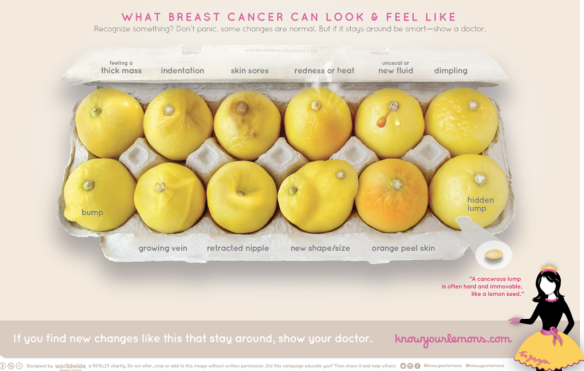 I wanted to share something I came across in the hopes it may be helpful to someone reading this. Please follow the link below to see what breast cancer can look & feel like. Remember, early detection is key!!!
I wanted to share something I came across in the hopes it may be helpful to someone reading this. Please follow the link below to see what breast cancer can look & feel like. Remember, early detection is key!!!